UNTERSUCHUNGEN
Beschreibung der klinischen Untersuchung des Ellenbogens.
Der Arzt, Therapeut oder medizinische Spezialist kann die klinische Untersuchung Ihres Tennisarms mit einer Ultraschalluntersuchung, einer MRI-, Röntgen- oder CT-Aufnahme erweitern. Wichtig ist dabei folgendes zu beachten: wenn Pathologie des Sehnengewebes festgestellt wird, heißt das noch nicht, dass diese Pathologie auch die Ursache der Beschwerden ist. Häufig gibt es die gleiche Pathologie auch am anderen Ellenbogen, wo es keine Beschwerden gibt. Die oben genannten Untersuchungen können dazu beitragen, das Stadium der Pathologie festzustellen. Sie können auch dazu dienen, sonstige Pathologie des Ellenbogens auszuschließen. Die Diagnose Tennisellenbogen kann durch Bewegungstests auf verlässliche Art gestellt werden. Weitere Untersuchungen sind deshalb nicht nötig. Eine Diagnose, die nur auf Bilder (“imaging”) gegründet ist, ist nicht immer verlässlich. Bewegungstests und Anamnese sind unerlässlich.
Bei den Bewegungstests des Tennisellenbogens ist kaum einen Unterschied zu machen zwischen den unterschiedlichen Muskeln die für die Beschwerden verantwortlich sind. Diese Muskeln haben einen gemeinsamen Sehnenansatz und jede Anspannung von einem der Extensoren hat direkte Folgen für die anderen. Auch durch Palpation kann ein Unterschied nicht auf verlässliche Art gemacht werden. Physiotherapeuten sind dazu geneigt, die Sehnenverletzungen des Tennisarms in die Kategorien 1 bis 4 einzuteilen. Diese Differentialdiagnose ist jedoch nicht verlässlich und führt bei der Behandlung zu keinen Konsequenzen. Die Pathologie eines Tennisarms ist ausschließlich im Gebiet der Übergang von Sehne zu Knochen zu lokalisieren. Die Stelle des Schmerzens ist nicht immer die Stelle der Pathologie.
The elbow complex is made up of three separate articulations, the humero-ulnar joint, the humeroradial (radiocapitellar) joint, and the superior radio-ulnar joint. These joints are covered by the same capsule. The elbow allows flexion and extension, as well as pronation and supination, and thus enables the hand to be placed in a variety of positions in space. Elbow flexion brings the hand to the chest, the mouth, or the face, thereby allowing the performance of most of the activities associated with feeding, dressing, and body care; elbow extension, on the other hand, takes the hand away from the body, and enables it to grasp objects. Elbow injuries are rare; however, they may be difficult to diagnose. This problem may be resolved to some extent or simplified by a full and systematic clinical examination. The joint is superficial, and hence readily accessible to clinical examination. As with other structures in the body, the examiner must be thoroughly familiar with the anatomy of the joint and with the abnormal conditions that may be encountered. This article deals with the broad principles of clinical examination, and will highlight only some of the disorders of the elbow.
ANATOMY AND PATHOPHYSIOLOGY
ANATOMICAL STRUCTURES
The anatomy of the elbow joint and the surrounding structures has been the subject of much research. In this article, only the main points that have emerged from recent studies will be summarized.
The bones (Figs. 1-4 )

Figure 1 Diagrammatic AP view of elbow joint
Figure 2 Diagrammatic lateral view of elbow joint.
Note that the elbow is slightly twisted in respect of the axis of the ulna.
The trochlea is shaped like a pulley; its medial lip is more prominent than the lateral one. The groove of the pulley runs obliquely downwards and outwards; it courses in a helical manner, forming an arch of about 330°. The distal joint surface of the humerus is in about 30° anterior rotation with respect to the long axis of the humerus, in the agittal plane; the condyles have 3-8° of internal rotation with respect to a line joining the epicondyles, in the axial plane; while, in the frontal plane there is a 6-8° valgus tilt of the condyles with respect to the long axis of the humerus(32, 34, 42). Elbow rotation is virtually around a single centre, which coincides with the condylotrochlear axis(48). On a true lateral radiograph of the elbow, the flexion-extension axis is at the centre of three concentric circles formed, respectively, by the projection of the edges of the condyles, the ulnar groove at the back of the medial epicondyle, and the medial lip of the trochlea (Fig. 4b). This flexion-extension axis is on a vertical line drawn down from the anterior cortex of the humeral shaft. It is an essential landmark for the implantation of a total elbow joint replacement
 Figure 3AP
Figure 3AP
radiograph of the elbow
 Figure 4a:
Figure 4a:
Radiograph ofthe elbow taken at right angles to the axis of the forearm.
Note medial rotation of the humerus, as shown in the diagram in Figure 2.
 Figure 4b:
Figure 4b:
True lateralradiograph of the humerus.The centres of the three circles formed by the edge of the condyle, the ulnar groove, and the medial lip of the trochlea coincide; this point is theflexion-extension axis of the elbow.The axis is on a vertical line drawn down from the anterior cortex of the humeral shaft.
There is a valgus angle of about 4° between the trochlear (greater sigmoid) notch of the ulna and the ulnar shaft (32, 34). The opening of the trochlear notch is angled ca. 30° posteriorly with respect to the long axis of the ulna; this allows better approximation in flexion to the 30° anterior rotation of the humeral articular condyles (34). The joint surface of the trochlear notchforms an arc of about 180°; however, it is not entirely covered with cartilage: in over 90% of individuals, a bare area covered by fibro-adipose tissue extends transversely across the mid-portion of the trochlear notch; this feature accounts for the frequency of fractures at this site, and permits a trans-olecranon approach to the joint (34). The radial head is covered with cartilage over four fifths of its circumference. The 15° angulation between the neck and the shaft of the radius leaves an excursion of 180° for forearm rotation(34).
The joint capsule
The capsule is attached around the articular surfaces, and blends with the annular ligament. It covers the tip of the olecranon, the coronoid process, and the radial fossa. The fibres are arranged in such a way as to provide stabilization in flexion and in full extension(23). When the elbow is stiff, the capsular capacity will be reduced by more than 50%; equally, the capsular compliance of the stiff elbow will be very poor, which shows that the capsule itself has been compromised(14). The position of minimum intracapsular pressure (“resting position”) is around 60-70° of flexion, which means that prolonged immobilization of the elbow in this position – as practised since the days of Ambroise Paré – will increase the risk of capsular contraction(14).
The ligaments
The medial collateral ligament is a strong and well-demarcated structure that consists of three bundles (Fig. 5):
Figure 5
Diagrammatic view of the medial collateral ligament, with its three bundles. The anterior bundle is the most important functionally, since it provides valgus and anteroposterior stability.
Figure 6
Diagrammatic view of the lateral ligament complex. It would appear that the most import structure is the lateral collateral ligament, which blends with the annular ligament. The lateral ulnar collateral ligament is indissociable from the lateral collateral ligament, at its attachment to the lateral epicondyle. Distally, it branches off, and attaches to the supinator crest. The role of the accessory lateral collateral ligament is poorly understood.
Figure 7 Diagrammatic view of the origin and insertion of anconeus, which covers the capsule and collateral ligaments on the lateral side.
The oblique anterior bundle is wide (5 mm) and thick. Its apex is attached to the front and the medial aspect of the medial epicondyle, of which it covers twothirds, and its base to the medial aspect of the ulna, just below the coronoid process(9, 32).This bundle is taut in flexion and in extension; its mean length is 27 mm(31, 32).
The oblique posterior bundle is less well defined. This broader structure is also attached low on the medial epicondyle, and inserts in a fan-shaped pattern overvirtually the entire margin of the trochlear notch of the olecranon. It is one of the structures that make up the cubital tunnel floor(9). This bundle is taut in flexion only; it is absent in many primates, which suggests that it is not a main stabilizer of the elbow(31, 53). The two bundles of the medial collateral ligament insert slightly posterior to the centre of rotation,which accounts for the fact that they are tauter in flexion than in extension(23). The oblique transverse ligament (sometimes referred to as the ligament of Cooper) is short, and does not appear to have a stabilizing role(31, 32). It extends from the posterosuperior portion of the trochlear notch to the coronoid process; itsorigin blends together with that of the anterior bundle(9). Like the posterior bundle, it contributes to the floor of the cubital tunnel. On the lateral side, there is no discrete collateral ligament in the strict sense of the term. Anatomical patterns vary widely, which is whythe description of the structures involved has been difficult, and why disorders of the lateral collateral complex may be hard to understand(31, 32, 42, 43). There are five ligamentous structures involved in the lateral stabilization of the elbow joint (Figs. 6, 7): The lateral (radial) collateral ligament attaches to the medial aspect of the lateral epicondyle and inserts into the annular ligament(31). Its origin overlies the centre of rotation of the elbow, which means that the ligament will be taut throughout flexionand extension(23, 32). Its mean length is 21 mm(31). The fan-shaped base of the ligament blends with the fibres of the annular ligament(43). The annular ligament is a thick structure that attaches to the anterior and posterior margin of the radial (lesser sigmoid) notch. It makes up four fifths of thefibro-osseous ring that encircles the head of the radius(32). The lateral ulnar collateral ligament is difficult to distinguish as a discrete structure. It attaches to the lateral epicondyle, like the lateral collateralligament, with which it blends at this site; it inserts into the superficial and posterior fibres of the annular ligament, but attaches to the supinator crest of the ulna(31, 42, 43). It forms, roughly, the posterior part of the lateral collateral ligament complex. The accessory lateral collateral ligament has its origin in the distal fibres of the annular ligament, and attaches distal to the attachment of the lateral ulnarcollateral ligament. It is an inconstant structure. Since it is taut only with varus stress, it may act as a stabilizer of the annular ligament when a varus stress is imposed upon thejoint(32, 42). The anconeus muscle, whose physiological role is still the subject of controversy, appears to be chiefly a joint stabilizer, serving as an active collateral ligament(7, 53). This would account for the fact that it is often torn when the lateral collateral ligamentcomplex is ruptured as a result of elbow dislocation.
BIOMECHANICAL IMPLICATIONS
About 60% of the axial loads imposed on the elbow will be transmitted through the humeroradial joint, as compared with only 40% through The humero-ulnar articulation(34). The stresses imposed on the elbow vary; they depend on the load applied, the resultant force vector, and the length of the lever arm. The loads may amount to 2-3 times the body weight, and to 8-10 times the lifted weight. This accounts for the compressive loads observed during simple activities such as dressing or feeding(48, 51). The use of crutches will transfer between 40% and 50% of the body weight onto the upper limb(51).The elbow is a very congruous joint, and, hence, inherently very stable. In flexion, the coronoid process locks into the coronoid fossa,
while the medial rim of the radial head engages in the trochleocapitellar groove(23). In extension, the apex of the olecranon is held in the olecranon fossa. Elbow stability is enhanced by the perfect congruency between the radial head and the radial notch of the ulna. Roughly speaking, the bony surfaces contribute 50% of the mediolateral stability of the elbow, while the other 50% comes from the ligaments(34). One important thing to bear in mind is that the role of each of these structures varies with the degree of flexion or extension of the elbow.Seventy-eight per cent of the valgus stability of the elbow is contributed by the medial collateral ligament; the bony surfaces, including the humeroradial joint, have only an accessory function in the constraint to valgus stress of the elbow, although experimental studieshave not as yet provided unequivocal evidence(19, 29, 33, 42, 48). In experiments, the insertion of a Silastic implant was seen to leave valgus stability unaltered(19). By and large, valgus stability comes from the bony structures below 20° and above 120° offlexion, and from the anterior bundle of the medial collateral ligament over the in-between range(11). The flexor-pronator group is bulky, but does not appear to provide dynamic support of the medial aspect of the elbow(16). The radial head has only a secondary role, providing about 30% of the stability on the lateral side(19, 23, 33). The minor importance of the radial head as a lateral stabilizer is illustrated byt he fact that radial head excision will not adversely affect the joint, providing that the medial collateral ligament is intact. However, a distinction must be made between elbow valgus stress, which is checked by the medial collateral ligament, and external rotation (or supination) stress, which is checked by the lateral collateral ligament(43). There is much less agreement concerning the roles of the different ligamentous structures in varus stability. Initially, it was thought that the annular ligament was chiefly responsible for resistance to varus stress between 40° and 60° of elbow flexion(49). According to this author, the lateral collateral ligament serves to stabilize the annular ligament. This idea was contested by several authors(48), which prompted Søjbjerg et al. to reinvestigate this subject. They showed that the isolated division of the lateral collateral ligament resulted in 15° of varus (at 110° of flexion), and that the division of the lateral ulnar collateral ligament had little influence on the instability observed(43). Thus, it is the lateral collateral ligament complex, and in particular the lateral collateral ligament, thatstabilizes to varus and extension loads(34, 43, 49). The sole function of the annular ligament appears to be the stabilization of the radio-ulnar joint. The anterior joint capsule resists distraction, and, under those conditions, provides 85% of the resistance observed(33). In the sagittal plane, stability also depends on the medial collateral ligament(33). Loss of less than 50% of the olecranon will not interfere with function, providing that the collaterals are intact(4). Valgus stability is provided largely by the proximal portion ofthe trochlear notch of the ulna (85%), while varus stability is chiefly a function of the distal part of this notch (65%)(4, 23). In the sagittal plane, bony stability in extension comes from the coronoid process(23, 47). This bony and ligamentous stability is enhanced, in the sagittal plane, by the powerful action of the muscles around the elbow.
CLINICAL EXAMINATION
HISTORY
In addition to the standard orthopaedic history, the following items of information should be obtained from patients presenting with elbow dysfunction: age, duration of the complaint, or time since onset of the elbow-related symptoms. The dominant side needs to be ascertained; specifically, it must be established whether there has been a recent reversal of the natural dominance, which would show that function has been severely impaired. The severity of the patient s pain is assessed using a visual analogue scale. The site of the pain may provide valuable clues. Conditions involving the lateral compartment (radiocapitellar joint) provoke pain that extends over the lateral aspect of the elbow, with radiation proximally to the midhumerus and distally over the forearm; this pain may be deep. Diffuse pathological conditions, on the other hand, cause pain that is described as periarticular in distribution(55) The patient should be questioned about locking, pain and/or instability during throwing movements, joint swelling, or fleeting inability to extend the elbow, which would suggest a joint effusion. Paraesthesiae of the hand may, in some cases, be related to ulnar nerve compromise at the level of the elbow. A note should also be made of any previous treatments of the elbow (synoviorthesis, intra-articular injections, surgery).
INSPECTION
Since the elbow is a superficial joint, many of its disorders can be readily detected by simple inspection. The patient should be suitably undressed to the waist for examination. Since, at the front, the muscle masses obscure the joint, much of the examination will need to be conducted with the examiner sitting or standing behind the patient. The patient should be standing, with shoulders slightly braced back, to display the elbow.
When the forearm is in full extension and supination, there will be a physiological valgus (“carrying angle”) of 9-14°; in women, the angle will be 2-3° greater (8, 18, 35, 55). This angle has been found to be 10-15° greater in the dominant arm of throwing athletes (5). This angle allows the elbow to be tucked into the waist depression above the iliac crest; it increases when a heavy object isbeing lifted (Fig. 8). Any increase in, or loss of, this physiological angle is indicative either of major elbow instability or of malunion. However, the angle varies from valgus in extension to varus in flexion, and its measurement is not of any practical importance(48).
 Figure 8
Figure 8
The physiological valgus ( carrying angle ) of the elbow is increased when a load is being carried. Normally, the angle is between 9 and 14° when the elbow is extended and the forearm is supinated. Sometimes, on the side of the elbow, bulging in the para-olecranon groove will be seen; such a swelling is produced by an effusion or by synovial tissue proliferation (55). On the back, prominence of the olecranon is a sign of posterior subluxation of the elbow, a feature commonly found in RA (55).
Rheumatoid nodules are extremely common; they are usually found on the posterior aspect of the elbow, mainly on the medial aspect of the extensor surface. The nodules should be counted and their volume noted: large nodules may cause skin ulceration and harbour infection. A note should also be made of their site, since they may cause problems if they are over an intended surgical approach to the elbow. Bursitis is also a frequently encountered pathology, especially in RA patients. As with nodules, the volume of the lesion and the quality of the overlying skin should be noted Inspection may also show skin atrophy at steroid injection sites, or scars from previous surgery. These features must be noted, since they may affect the surgical approach to be employed.
PALPATION
Palpation starts at the posterior aspect, with the patient standing with his or her shoulder braced backwards. The three palpation landmarks – the two epicondyles and the apex of the olecranon – form an equilateral triangle when the elbow is flexed 90°, and a straight line when the elbow is in extension (Figs. 9, 10).

Figures 9, 10
Three bony landmarks – the medial epicondyle, the lateral epicondyle, and the apex of the olecranon – form an equilateral triangle when the elbow is flexed 90°, and a straight line when the elbow is in extension
Since the elbow is a very superficial joint, it can be readily palpated from behind and from the sides. The posterior aspect has the olecranon mid-way between the medial and the lateral condyle. Slight elbow flexion will bring the olecranon out of the olecranon fossa, in which it lodges in extension; in this position, the proximal portion of the fossa on either side of the triceps tendon may bepalpated (Fig. 11).
 Figure 11
Figure 11
Flexing the elbow allows palpation of the olecranon fossa on either side of the triceps tendon.
 Figure 12
Figure 12
Anatomical landmarks on the lateral aspect of the elbow: The lateral epicondyle continues proximally in the supracondylar ridge. Two centimetres distally, the main landmark is formed by the radial head.
The olecranon bursa is not in communication with the synovial cavity. This is why the elbow may be mobilized in bursitis, and why even massive bursitis will not be tender. In chronic bursitis, a boggy globular mass may be palpated; the overlying skin will be thickened. Flat, hard nodules may be felt under the palpating fingertips(12). In infected bursitis, the skin will be tight and shiny; streaks of lymphangitis will be commonly seen; while in 25% of the cases, the axillary lymph nodes will be enlarged(12). On the lateral side, the main landmarks are the lateral epicondyle proximally and the radial head distally. The supracondylar ridge is also very accessible to palpation; its chief value is that of a landmark for surgical approaches (Fig. 12). Sometimes, palpation may be carried out all the way up to the deltoid tuberosity. The radial head is palpated with the examiner s thumb, while the other hand is used to pronate and supinate the forearm (Fig. 13). The head is about 2 cm distal to the lateral epicondyle(5). Inside the triangle formed by the bony prominences of the lateral epicondyle, the radial head and the olecranon, the joint itself is palpated, to detect even very minor effusions or low-grade synovitis (Fig. 14).
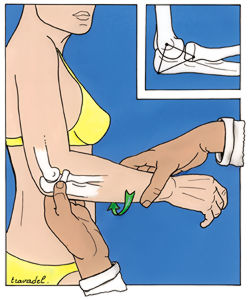 Figure 13
Figure 13
Anatomical landmarks on the lateral aspect of the elbow: The radial head is palpated with the thumb, while the examiner s other hand is used to pronate and supinate the forearm.
Figure 14
Theelbow joint may be palpated inside a triangle formed by the bony prominences of the lateral epicondyle, the radial head, and the olecranon. This palpation will reveal even minoreffusions or mild synovitis. Puncture for joint aspiration is performed inside this triangle. Similarly, an arthroscopy portal may be placed there (posterolateral portal).
The muscles on the lateral side may be palpated individually. For the palpation of brachioradialis, the patient is asked to clench his orher fist and flex the elbow with the forearm in neutral position (mid-way between pronation and supination) and with the fist blocked under a table (Fig. 15). The wrist extensors are palpated by asking the patient to extend the forearm at the elbow against resistance (Fig. 16). Extensor carpi radialis longus produces both flexion and abduction of the wrist. Anconeus may be palpated behind the radial head, on the side of the olecranon; it increases in bulk when the forearm is extended against resistance(35).

Figure 15
Palpationand testing of brachioradialis, a forearm flexor.

Figure 16
Palpation and testing of the wrist extensors
From the medial side, the joint is not very accessible to palpation, and the small amount of synovial tissue on the medial border of the olecranon makes joint palpation difficult(35). Palpation of the ridge that provides insertion for the intermuscular septum is useful mainly as a guide for surgical approaches. Also, the supracondylar lymph nodes may be palpated at this site (Fig. 17). Over, and slightly anterior to, the supracondylar ridge, a bony excrescence may be palpated; this outgrowth may irritate the median nerve(5). This supracondylar process is present in 1-3% of the population, and is seen at a distance of 5-7 cm above the joint line(32). Behind the septum, the ulnar nerve may be palpated; in patients with a very mobile nerve, it may be seen to roll on the medial condyle(10)(Fig. 18). Ulnar nerve instability is more easily tested with the arm in slight abduction and external rotation, with the elbow flexed between 20 and 70°.
 Figure 17
Figure 17
Palpation of the medial aspect of the elbow. Above the medial epicondyle is the ridge on which the intermuscular septum inserts. Two centimetres above the epicondyle is the site used for lymph node palpation.
 Figure 18
Figure 18
The ulnar nerve is palpated behind the intermuscular septum. It may sometimes sublux or roll on the epicondyle. Ulnar nerve instability is more readily demonstrated if the elbow is flexed 60° and the upper limb is abducted and externally rotated.
Anteriorly, the bulk of the flexor-pronator group restricts the extent of joint palpation. The flexor-pronator muscles must be tested as a unit, by asking the patient to perform wrist adduction and flexion against resistance (Fig. 19). Next, each one of these muscles should be tested individually. The anterior aspect does not lend itself to palpation, since it is tucked away behind the muscles. Laterally, brachioradialis will be felt; and in the middle, the biceps tendon is readily accessible if the patient is made to flex the forearm against resistance. Lacertus fibrosus is palpated medial to the biceps tendon; the pulse of the brachial artery will be felt deep to this aponeurosis (Fig. 20). Sometimes anterior protrusion cysts produced by herniated synovial membrane may be felt(52).
 Figure 20
Figure 20
Palpation of the medial biceps expansion (lacertus fibrosus), which courses over the brachial vessels and the median nerve.
 Figure 19
Figure 19
Diagrammatic view of the pattern of the flexor-pronator group: The thumb represents pronator teres; the index, flexor carpi radialis; the middle finger, palmaris longus; and the ring finger, flexor carpi ulnaris.
MOBILITY
The main function of the elbow is to bring the hand to the mouth; this is why the investigation of the elbow range of movement (ROM) is an important part of the examination process. Any difference between passive and active mobility is usually due to reflex inhibition from pain(55). The end-feel – the feeling transmitted to the examiner s hands at the extreme range of passive motion – must also be assessed (Table 1). If the feel is abnormal, there is usually something wrong with the joint.
Bony Two hard surfaces meeting, bone to bone (elbow extension)
Capsular Leathery feel, further motion available (forearm pronation and supination)
Soft tissue approximation Soft tissue contact (elbow flexion)
Spasm Muscle contraction limits motion
Springy block Intra-articular block; rebound is felt
Empty Movement causes pain, pain limits movement
Table 1 Classification and description of end-feels (modified from TS Ellenbecker & AJ Mattalino)(12a)
Flexion-extension
The normal flexion-extension range is 0 to 140° (+ 10°). Mobility is measured with a goniometer placed on the side of the arm and forearm; the measurement thus obtained will be reliable to within 5° of accuracy(35) (Fig. 21). This ROM is well in excess of what is needed for the majority of activities of daily living (ADLs). The useful arc of motion is between 30° and 130° of elbow flexion; most ADLs require an arc of only 60-120°(30, 33, 55) (Fig. 22).

 Figure 21a-b
Figure 21a-b
Flexion-extension is measured with a goniometer applied to the lateral aspect of the elbow. The normal range is 0-140° (+ 10°).
 Figure 22
Figure 22
Arcs of flexion required for some activities of daily living (adapted from Morrey, 1981) Door / Chair / Fork / Telephone
Loss of extension provides a very sensitive clue to intra-articular elbow pathology, since extension is the first sector of the ROM to be affected, and the last to recover(55). However, since the extension deficit shortens the lever arm, it is well tolerated up to a loss of 45°(55). At the end of flexion, there will be a soft-tissue approximation end-feel as the movement is blocked by the bulk of the arm and forearm muscles. At the end of the normal extension movement, there will be a bony end-feel, as the olecranon locks into the olecranon fossa(5).
Pronation and supination
Pronation and supination cannot be complete unless the proximal and distal radio-ulnar joints are in correct anatomical relationship, the two bones are of normal length relative to each other, and the interosseous membrane is intact(55). The arc of motion varies widely in different individuals; the mean values are 70° pronation, and 85° supination (Figs. 23, 24). However, with only 50° pronation as well as supination, most ADLs can be readily performed(30, 55). At the end of pronation and supination, there will be a capsular end-feel(5).
 Figure 23 Measuringpronation: The vertical limb of the goniometer is placed parallel to the long axis of the humerus, while the horizontal limb is placed on the back of the wrist (to eliminate additionalmotion at the radiocarpal joint). The mean value is 70°.
Figure 23 Measuringpronation: The vertical limb of the goniometer is placed parallel to the long axis of the humerus, while the horizontal limb is placed on the back of the wrist (to eliminate additionalmotion at the radiocarpal joint). The mean value is 70°.
 Figure 24Measuring supination: The horizontal limb is placed on the anterior aspect of the wrist. The mean value is 85°.
Figure 24Measuring supination: The horizontal limb is placed on the anterior aspect of the wrist. The mean value is 85°.
STABILITY
Mediolateral stability
Stability testing is performed with the patient standing, shoulder braced backwards; the examiner is behind the patient. The elbow is slightly flexed, to bring the apex of the olecranon out of the fossa. Varus stability is checked with the humerus in full internal rotation, while valgus stability is tested in full external rotation (Figs. 25, 26). The physiological laxity of the elbow between 10 and 20° of flexion, in varus and in valgus, does not exceed 5°. In rotation (pronation and supination), it does not exceed 3°(49).
 Figure 25a-b
Figure 25a-b
Testing mediolateral elbow stability
25a:
To eliminate interfering movements during varus instability testing, the humerus is placed in fullinternal rotation and the forearm in pronation.
 25b:
25b:
To eliminateinterfering movements during valgus instability testing, the humerus is placed in full external rotation. Valgus testing is done with the forearm pronated, to test the medial collateralligament, followed by testing in supination, to check the lateral collateral complex.
 Figure 26
Figure 26
Testing mediolateral stability in an RA patient with a TEJR
26a: Varus instability
 26b:
26b:
Valgusinstability. The physiological mediolateral instability is < 5°.
Patients may also be examined lying supine. In this case, the humerus is held with one hand, while the examiner s other hand places the forearm in valgus (or in varus), with the elbow flexed 20-30° (to remove the olecranon from the fossa)(5, 39) (Fig. 27). With the patient s abducted and externally rotated arm tucked under the examiner s shoulder, the medial collateral ligament may be palpated at the same time(11) (Fig. 28). As we shall see in the section on instability, it is important for mediolateral stability to be tested in pronation and in supination.
 Figure 27
Figure 27
Assessing mediolateral stability with the patient lying supine. The elbow should be slightly flexed, to disengage the olecranon from the fossa. Testing must be done in pronation and in supination.
 Figure 28
Figure 28
With the abducted and externally rotated arm tucked under the examiner s shoulder, the medial collateral ligament may be palpated.
Anteroposterior stability
Anteroposterior stability is controlled exclusively by the collaterals. Removal of the olecranon will not result in instability if the collaterals, and above all the medial collateral ligament, are intact. In RA patients, a search should be made for anteroposterior translation, which shows the extent of joint destruction. The forearm is flexed to 90° and held by the examiner with one hand, while the other hand holds the humerus, as anteroposterior stress is applied to the joint.
NEUROLOGICAL EXAMINATION
This examination forms part of the examination of the elbow; depending on the patient s symptoms, a rough screen or a more detailed investigation will have to be performed.
Ulnar nerve
At the elbow, the ulnar nerve may be damaged at several different levels: at the arcade of Struthers; in the ulnar groove behind the medial epicondyle; under the fascial band bridging the two heads of flexor carpi ulnaris (arcade of Osborne); and even under the deep aponeurosis of flexor carpi ulnaris(3) (Figs. 29, 30). Tinel s sign, elicited at different levels, will give a clue as to the site of the compression (Fig. 31).
 Figure 29
Figure 29
Diagrammatic view of the four zones around the elbow in which the ulnar nerve may be compressed
1- Under the deep aponeurosis of flexor carpi ulnaris
2- Under the fibrous arcade formed by the two heads of flexor carpi ulnaris (arcade of Osborne). This is the most frequently encountered entrapment site.
3 – Behind the medial epicondyle
4 – At the arcade of Struthers
 Figure 30a-b
Figure 30a-b
Ulnar nerve compression in an RA patient.
30a: Ulnar nerve (on loop) flattened by synovial proliferation, and destruction of the joint.
 30b: With the nervepulled out of the way, the inflamed synovia is seen at the bottom of the tunnel.
30b: With the nervepulled out of the way, the inflamed synovia is seen at the bottom of the tunnel.
Figure 31
 Eliciting Tinel’s sign: Paraestesiae in the territory of the ulna nerve allow an assessment of the likely site ofcompression
Eliciting Tinel’s sign: Paraestesiae in the territory of the ulna nerve allow an assessment of the likely site ofcompression
In the ulnar groove, the ulnar nerve may be affected by synovial proliferations herniating on the medial side of the joint; by bony lesions with spicules causing irritation along the course of the nerve behind the epicondyle; or by ischaemic events. Paraesthesiae of the ulnar border of the hand and the fingers are usually the first signs of ulnar neuropathy. Pain is a less frequent complaint; where it is encountered, it is usually localized to the elbow or along the medial edge of the forearm. These symptoms are commonly triggered or exacerbated by attempts to flex the elbow. Prolonged elbow flexion may produce the paraesthesiae reported by the patient. This test – known as the elbow flexion test, and analogous to Phalen s test for carpal tunnel syndrome – can be made more discriminating by putting the wrist in extension, so as not to perform a Phalen test at the same time. In the more advanced stages, there will be ulnar nerve palsy as well.
Posterior interosseous nerve
The posterior interosseous nerve is the motor branch of the radial nerve. It can be found, at the back of the arm, using the three-finger method described by Henry: the index, middle, and ring fingers of the examiner s hand opposite the examined side are placed on the posterior aspect of the radius, with the ring finger at the junction between the neck and the head of the radius. The nerve will then be under the tip of the index finger.
Anterior interosseous nerveThis motor branch of median nerve origin may be compressed where it courses between the two heads of pronator teres(17). Compression of this nerve will lead to weakness and even paralysis of the flexor digitorum profundus muscle of the index finger and the flexor pollicis longus muscle of the thumb. The patient will be unable to create an OK sign (pinching the tips of the index finger and the thumb together).Global muscle evaluation Testing the different muscles around the elbow forms part of the standard workup of patients with elbow complaints. Each muscle must be tested separately. Details of the technique to be employed will be found in the standard textbooks, such as Kendall s(22). The global evaluation gives a picture of the extent of a nerve trunk or plexus lesion. Table 2 lists the actions, nerve supply, and nerve root derivations of the different muscles.
Reflexes
Testing the reflexes forms part of the neurological examination of the elbow. The biceps reflex is a C5 function (although the muscle is supplied by C5 and C6); the brachioradialis reflex is C6; and the triceps reflex, C7 (Figs. 32, 33, 34).


 Figures 32, 33, 34
Figures 32, 33, 34
Testing the biceps reflex (Fig. 32 – C5 root)
brachioradialis reflex (Fig. 33 – C6 root)
triceps reflex (Fig. 34 – C7 root)
FUNCTIONAL TESTING
Functional investigation of the elbow Pronator, supinator, and extensor strength is largely the same on the dominant and the non-dominant side; this is why a comparison with the unaffected side is the best test(13). However, flexor strength is always greater on the dominant side. A manual assessment of elbow strength, at 90° of flexion and with the forearm in neutral position, may appear somewhat crude. However, this isometric measurement is very reliable, yielding values close to the results of isotonic measurements, which are much more difficult to perform(6). Male subjects are about twice as strong as females, and the dominant limb is about 6% stronger than the non-dominant one(6). Extensor strength is about 60-70% of flexor strength(6, 35, 55). Supinator strength usually exceeds pronator strength by 15%(6, 35, 55). Strength must be assessed, especially in RA, because of the magnitude of mechanical stresses: a 1 kg weight at the hand produces a reactive force, at the 90° flexed elbow, of the order of 10 kg(55).
Functional investigation of the upper limb
The elbow is situated between two highly mobile joints – the shoulder and the wrist. It can compensate only for flexion-extension deficits. As regards flexion, the overall capability for feeding (hand to mouth), body care (hand to face), and hair care (hand to back of head) should be examined. The activities looked at with regard to extension are opening doors, and reaching to grasp objects. Global functional investigation: the lower limbs – walking aids. A search must be made for coexisting conditions affecting the lower limbs. The use of walking aids puts increased functional loads on the elbow, and may rule out elbow joint replacement. On the other hand, a hip or knee condition may have to be treated with surgery first, before doing elbow replacement, so as not to jeopardize the outcome of the elbow arthroplasty.